
Approximate Read Time: 8 Minutes
“Platelet Rich Plasma (PRP) is not a single therapy but a spectrum of biologics. Its history, preparation, and application determine whether it heals or disappoints.”
What You Will Learn
- PRP is not a single treatment but a spectrum of biologics.
- Evidence supports PRP in osteoarthritis and tendon injuries.
- Outcomes depend on preparation, injury type, and physical therapy.
The Promise and the Problem
When platelet-rich plasma (PRP) first arrived in sports medicine, it was packaged as a breakthrough. A simple injection drawn from an athlete’s own blood that promised to heal tendons, cartilage, and joints. Early media coverage turned it into a miracle cure, with headlines about star athletes flying overseas to receive it. But the reality, two decades later, is more complicated.
The problem is not that PRP doesn’t work. It’s that not all PRP is created equal. There isn’t one PRP, but dozens of variations, each with unique biological signatures. As Dr. Chuck Peterson and Dr. Cam Davis noted in our conversation, PRP was the “entry point” for orthobiologics, but it has suffered from inconsistency. Without standardization, outcomes have been as varied as the products themselves.
To understand PRP today, we need to look at its history, its many forms, where it helps, where it fails, and how rehabilitation integrates to determine whether the biology translates into performance.
A Brief History of PRP
PRP began in hematology and dentistry. In the 1970s and 1980s, oral surgeons used platelet concentrates to speed wound healing. By the early 2000s, PRP made its way into orthopedics and sports medicine. Professional athletes were among the first high-profile recipients, which fueled hype well beyond the science.
PRP is the “first-generation biologic.” It opened the door for regenerative medicine in sports but quickly revealed its limitations. Clinics competed to market PRP without always disclosing what type they used, how it was processed, or which injuries it was best suited for. Unlike a pharmaceutical drug, which is chemically identical every time, PRP is a process. That means two clinics can prepare PRP differently and end up with two entirely different products under the same name.
“Standardization in PRP preparation is urgently needed, as variability between clinics explains why some patients thrive while others see no benefit.”
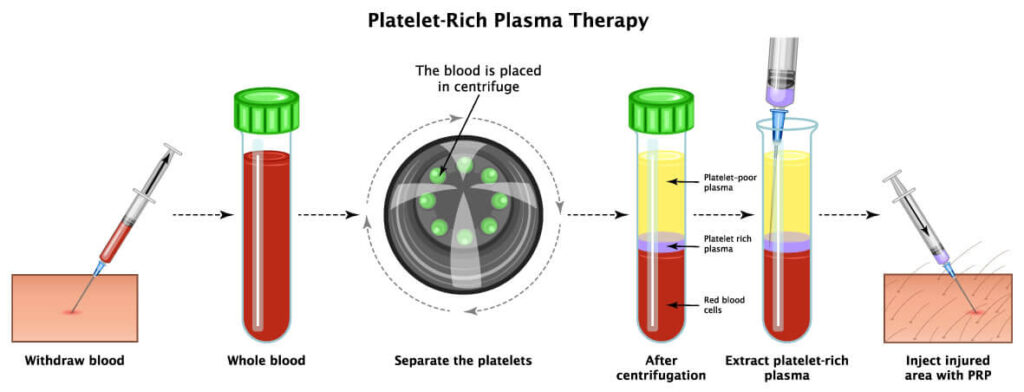
What is PRP? The Science Behind the Syringe
PRP is blood plasma with a higher concentration of platelets than baseline. Normally, platelets circulate to clot blood. But inside their granules are growth factors and cytokines that signals the body to promote tissue repair, angiogenesis, and inflammation resolution.
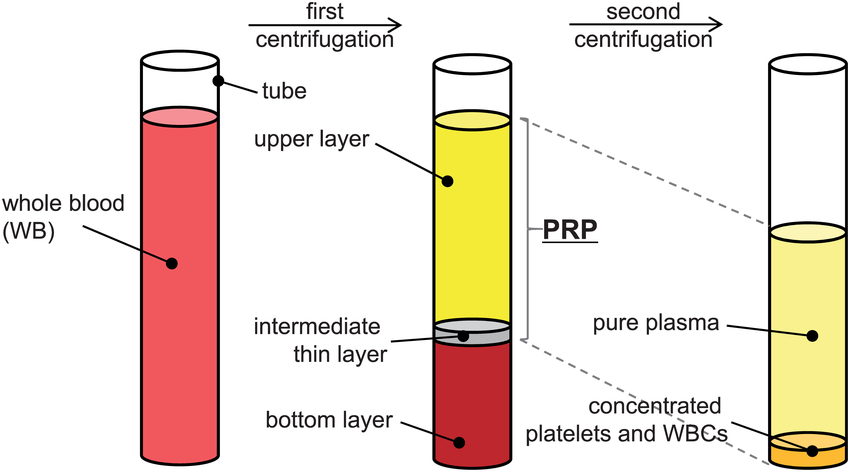
When concentrated and reinjected into tissue, PRP is thought to accelerate or amplify the body’s natural healing cascade. But the exact cocktail of growth factors depends on how the PRP is prepared. Centrifuge speed, number of spins, inclusion or exclusion of leukocytes (white blood cells), and the final platelet concentration all dramatically change what ends up in the syringe (NBA Orthobiologic Consensus Statement, 2020).
This is why one PRP treatment might reduce knee pain and restore function, while another, marketed with the same acronym, produces little to no improvement.
FREE DOWNLOAD
Start Optimizing Your Stem Cell Recovery Today with this Recovery Guide!
The Many Faces of PRP
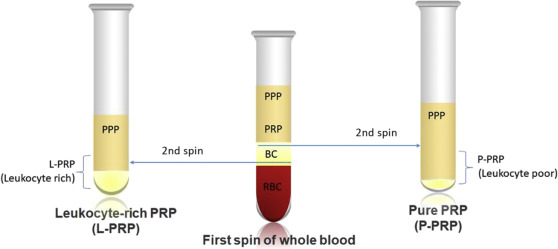
Leukocyte-Rich vs. Leukocyte-Poor
The biggest divide in PRP preparation is whether leukocytes are included.
- Leukocyte-rich PRP (LR-PRP): Contains more white blood cells, producing a stronger inflammatory response. This may be helpful in tendon pathology, where the goal is to restart a stalled healing process.
- Leukocyte-poor PRP (LP-PRP): Removes most leukocytes, creating a cleaner product with less inflammation. This is typically favored for intra-articular injections in osteoarthritis (Arundale et al., 2020).
Other Variations
- Single vs. double spin centrifuges produce different platelet concentrations.
- Additives: Some protocols combine PRP with hyaluronic acid (HA) for cartilage, or with bone marrow aspirate concentrate (BMAC) for complex injuries.
- Activation: Some clinicians “activate” PRP with calcium chloride or thrombin before injection, while others inject unactivated PRP.
In short, PRP is not one therapy rather it’s a family of biologics. Two patients receiving PRP at different clinics may be receiving fundamentally different products.
Where PRP Works
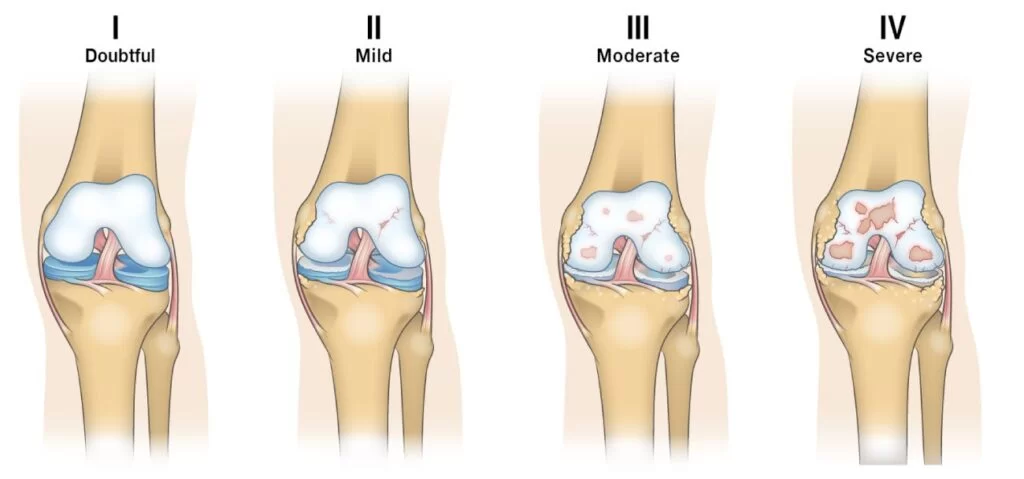
Osteoarthritis
Knee osteoarthritis is the most common use for PRP. Multiple trials have shown LP-PRP improves pain and function compared to placebo or hyaluronic acid in mild-to-moderate OA (Laver et al., 2020). Results are less robust in advanced disease, where joint structure is too far deteriorated.
Tendon Injuries
Evidence is strongest for tendinopathies. Lateral epicondylitis (“tennis elbow”) and patellar tendinopathy both respond well to LR-PRP, with improved pain and function compared to corticosteroids or placebo.
Muscle Injuries
PRP has been studied in hamstring strains among professional soccer players. While some studies suggest faster return to play, systematic reviews show mixed results. It may help with healing quality, but does not always shorten timelines (Maffulli et al., 2019).
Ligament Sprains and Meniscus
PRP is being applied to ACL graft maturation, MCL sprains, and meniscus healing. Results remain variable, and these uses are more experimental.
A study in elite football (soccer) showed PRP was commonly used for muscle and ankle injuries. Players reported mixed experiences, with some returning quicker and others seeing no clear benefit (Orchard et al., 2020).
Where PRP Falls Short
PRP is not universally successful.
- Advanced osteoarthritis: Little long-term benefit, especially with bone-on-bone degeneration.
- Large or complete tendon tears: PRP cannot replace surgical repair when tissue continuity is lost.
- Labral and intra-articular cartilage lesions: Evidence is weak and inconsistent.
The NBA Consensus Statement emphasized that many early PRP studies were underpowered, poorly standardized, and easily overinterpreted. Too often, clinics marketed PRP as a cure-all, which it is not (NBA Consensus, 2020).
PRP vs. Other Orthobiologics
Compared to newer biologics like stem cells, exosomes, peptides the PRP is basic. It is “the starting line” of orthobiologics. Stem cells and exosomes offer more regenerative potential, but are also more expensive, less regulated, and less accessible.
PRP remains popular because it is autologous (from the patient’s own blood), relatively inexpensive, and has a strong safety profile. For many athletes, it is the most pragmatic entry point into biologics.
Physical Therapy After PRP
“PRP alone doesn’t restore function. Rehabilitation guides the tissue’s new biology into performance.”
The injection itself is only the spark. Rehabilitation is the fuel that guides how that biology manifests in function.
Early Phase (Days 1–3)
Relative rest, activity modification, and pain modulation. The goal is to let the biologic “set” and do its thing.
Intermediate Phase (Week 1–3)
Gradual reintroduction of mobility and controlled loading. For tendons, this often includes isometrics progressing to slow eccentrics. For joints, gentle weight bearing and closed-chain exercises.

Advanced Phase (Week 3–6)
Progressive strengthening, higher load eccentrics, and neuromuscular training. Integration of kinetic chain to support the healing tissue.
Return-to-Performance (6+ Weeks)
Sport-specific drills, plyometrics, and exposure to chaotic environments. The injection created the biology; therapy restores the movement.

Practical Recommendations
For athletes, physical therapists, and clinicians:
- Ask what type of PRP is being used. LR vs LP matters.
- Set realistic expectations. PRP is not a cure-all.
- Use in the right context. Tendinopathy, mild-to-moderate OA, and select muscle injuries have the strongest evidence.
- Pair with structured rehab. Without it, PRP’s biological potential is wasted.
Conclusion: Beyond the Acronym
“PRP is valuable, but only when matched to the right injury, the right preparation, and the right rehabilitation.”
The story of PRP is one of promise complicated by variability. It is not a single therapy but a category. Its effectiveness depends on how it is prepared, where it is used, and how it is integrated with physical therapy.
PRP opened the door for orthobiologics. It is not the finish line, it was the starting gun.
FREE DOWNLOAD
Start Optimizing Your Stem Cell Recovery Today with this Recovery Guide!
Read More Like This

Related Podcasts

References
Laver, L., Cole, B., Arundale, A. J. H., Bytomski, J., & Amendola, A. (2020). Basketball sports medicine and science.Springer. https://doi.org/10.1007/978-3-662-61070-1
Maffulli, N., Randelli, F., Longo, U. G., Locher, J., Loppini, M., Denaro, V., & Cabitza, P. (2019). Utilization of orthobiologics by sports medicine physicians. Journal of Orthopaedic Surgery and Research, 14(1), 399. https://doi.org/10.1186/s13018-019-1482-8
National Basketball Association. (2020). NBA Orthobiologics Consensus Statement. Orthobiologics use in the NBA.
Orchard, J. W., Arundale, A., & Newman, P. (2020). Injectable orthobiologics in professional football players. British Journal of Sports Medicine, 54(9), 527–528. https://doi.org/10.1136/bjsports-2019-101245
Peterson, C., & Davis, C. (2024). Stem cells, exosomes, peptides, and orthobiologics. [Podcast transcript]. Finding Small Wins Podcast.


