
Approximate read Time: 6 minutes
“Exosomes are the delivery trucks filled with blueprints and project managers. Peptides are the actual tools and raw materials.”
What You will learn
- Peptides and exosomes are emerging tools in orthobiologics, bridging the gap between rehab and regeneration.
- Expert insights from Dr. Chuck Peterson and Dr. Cam Davis clarify their evolving clinical use.
- Peptides and exosomes can enhance, not replace, smart rehab and movement retraining.
The Landscape Is Expanding, But So Is the Confusion
Platelet Rich Plasma (PRP) changed the conversation. Stem cells shifted it again. And now? Peptides and exosomes are becoming more regular household terms.
But with newer interested into these therapies comes a common challenge: hype without clarity. People hear the terms on podcasts or from pro athletes, but don’t know what these tools actually do or how they differ from the last generation. Or how to effectively evaluate which may be best for them.
To make this article digestible, we’ll lean into a worksite analogy:
- PRP = the alarm system and cleanup crew
- Stem cells = the general contractors
- Exosomes = delivery trucks filled with blueprints and project managers
- Peptides = the actual tools and raw materials
Let’s explore what these biologics are, how they’re used, and what to know before you consider them.
From PRP to Stem Cells: How We Got Here
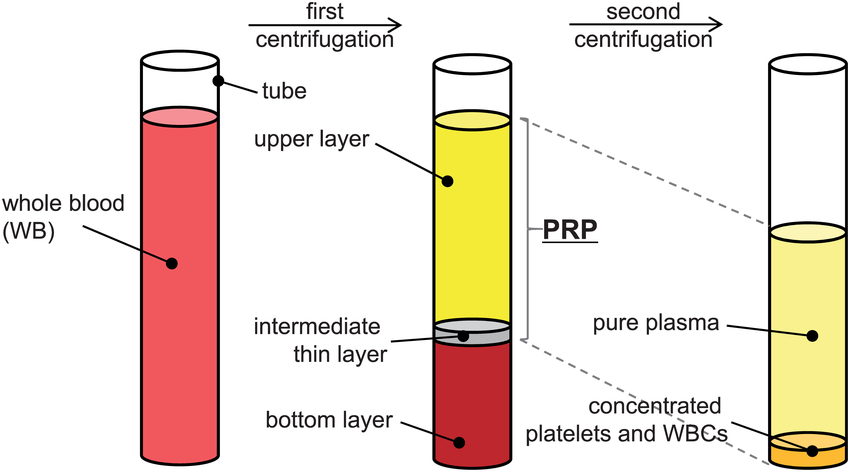
PRP (platelet-rich plasma) was the starting point. A simple blood draw and spin to concentrate healing factors. It works by initiating inflammation, cleaning up tissue damage, and kickstarting the repair process.
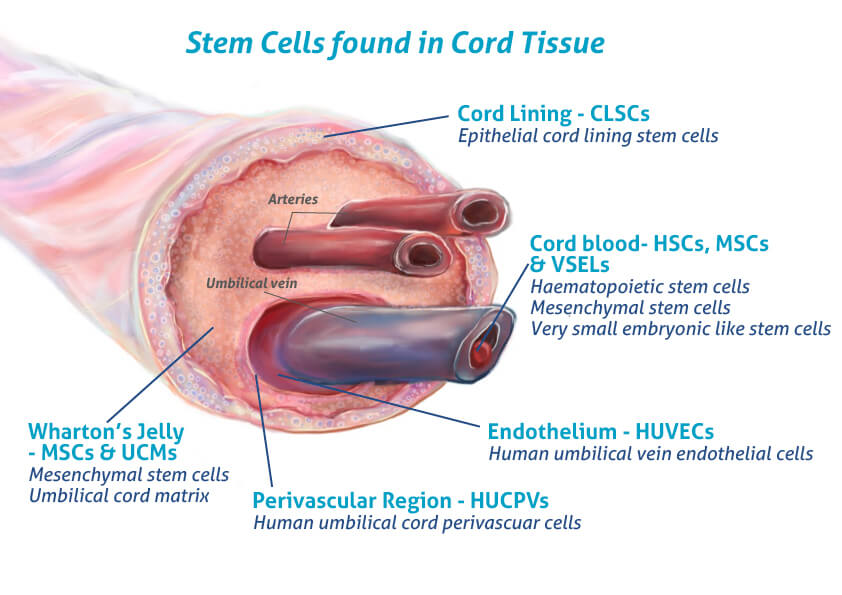
As stem cell science emerged, we began to isolate more potent healing agents using bone marrow aspirate concentrate (BMAC) and mesenchymal stem cells from umbilical cords. These came with more complexity, cost, and sometimes confusion.
For a deeper understanding, you can check out these other articles too:
- The Evolution of PRP
- How Stem Cell Therapy Supports Healing and Performance
- Regeneration Meets Rehab in Panama
What Are Exosomes?
Exosomes are small, bubble-like structures released by cells especially stem cells. Inside these microscopic vesicles are powerful cargo: proteins, mRNA, and microRNA that tell other cells what to do.
“Exosomes are like the text messages your body sends to coordinate healing.”
They’re messengers, not builders. They deliver information that directs your cells to reduce inflammation, grow new tissue, or clean up debris.

Benefits:
- No nucleus = lower risk of immune rejection
- Easier to produce and store than full stem cells
- Can be used systemically (IV) or locally (injection)
What Are Peptides?
“Peptides are tools you bring to the job site, but they don’t magically build the house.”
Peptides are short chains of amino acids that act primarily as signals in the body. Some function like messengers (turning pathways up or down). Others mimic hormones or regulatory proteins. That’s why “peptide therapy” sounds precise: you’re trying to influence biology using biology’s own language.
But a crucial distinction matters:
- Some peptides are real medicines that FDA-approved, standardized, and tested in humans (think insulin or GLP-1 medications).
- Many “wellness” peptides are often used off-label, compounded, or sold in gray-market channels with limited human data and unclear long-term safety.
The most talked-about peptide: BPC-157 (not “BP-157”)
BPC-157 is the poster child for modern peptide hype because the preclinical story is loud. Across animal and cell studies, BPC-157 has been associated with “repair-like” signaling in multiple tissue models tendon, muscle, ligament, nerve, bone, and GI tissue.
Mechanistically, the literature often points to pathways tied to:
- angiogenesis and vascular signaling (VEGF-related pathways),
- nitric oxide signaling, and
- cell migration / fibroblast activity involved in tissue remodeling.
Here’s the scientific bottleneck: human evidence remains extremely thin. Recent reviews in sports medicine and musculoskeletal contexts consistently emphasize that most published BPC-157 studies are animal-based, with minimal clinical-grade human data and no robust randomized controlled trials establishing efficacy or long-term safety.
And then there’s the regulatory reality: the FDA has specifically flagged BPC-157 on its list of bulk drug substances that may present significant safety risks when used in compounding, citing concerns like immunogenicity and issues tied to peptide impurities. So the cleanest, most accurate framing is:
BPC-157 has intriguing biological signals in preclinical research, but it has not earned the “proven therapy” label in humans yet.
Therapeutic Peptide Delivery
When it comes to reliably delivering peptides, injection remains the practical standard through subcutaneous, intramuscular, and sometimes intravenous. The reason is because peptides can have a short shelf-life. Many are quickly degraded by enzymes and face major absorption barriers in the GI tract.
That said, delivery science is evolving fast and this is where your section can feel modern without overpromising.
Injections: still the most predictable route
Injectables bypass most of the stability and absorption problems that oral peptides face. They also reduce “dose ambiguity” (what actually gets into circulation).
Some clinics also use extended-release approaches to reduce frequent dosing, although availability and evidence vary widely by compound and formulation.
Oral delivery: improving, but still a major hurdle for most peptides
Oral peptide delivery is a popular choice because it’s convenient, but it’s hard for two reasons: breakdown (stability) and poor intestinal permeability (absorption). Modern reviews describe strategies like absorption enhancers, enzyme inhibitors, protective carriers (lipid/polymer systems), and even “device-like” delivery concepts designed to help peptides survive and cross barriers.
Important nuance: the fact that some peptides can be made orally deliverable does not mean any clinic peptide can. Oral success tends to require very specific formulation engineering and validation.
Intranasal delivery: promising, but formulation dependent
Intranasal delivery is attractive because it’s noninvasive and can offer faster absorption for certain molecules, but it still struggles with mucosal barriers, clearance, and dose limitations.
Transdermal and other routes
Transdermal and other alternative routes remain limited for many peptides due to molecular size, skin barriers, and inconsistent absorption. This pathways is better described as research or frontier option than a go-to clinical decision in comparison to injection-based peptides options.
The bottom line
Delivery route is not a minor detail because it’s the difference between “biologically plausible” and “clinically meaningful.” And when peptides are sourced through poorly controlled channels, the delivery conversation becomes secondary to the more basic question: Is this even pure, sterile, and accurately dosed?
Am I optimistic and believe peptides are meaningful? Yes, and that comes with an asterisk around sourcing, quality, and viability of the product.
Insights from the Experts: Dr. Chuck Peterson & Dr. Cam Davis
In a recent episode of Finding Small Wins, I sat down with two of the leading voices in sports orthobiologics in the Arizona area, Dr. Chuck Peterson and Dr. Cam Davis.
We covered:
- Why inflammation isn’t the enemy and that it’s part of healing
- The difference between “treatment” and “cure”
- Why choosing the right intervention depends on your goals, age, and expectations
- Ethical considerations and financial realities in the U.S. vs abroad
🎧 Listen to the full conversation
What’s on the Horizon?
Imagine 3D-printed cartilage grown with your own cells embedded with biologics and scaffolded with cells is the hope that Chuck and Cam both envision this future.
The goal isn’t eternal youth. The hope is that it is precision repair that allows people to live, move, and train longer with less surgical intervention.
Until then, the goal is to slow degeneration, not just mask symptoms.
Final Thoughts: Precision, Not Promises
Peptides and exosomes aren’t magic. But they are powerful tools when used wisely. They work best when paired with:
- Rehab that respects the biology of tissue healing
- Movement strategies that offload stress and restore coordination
- Patient education that reframes expectations
“You can’t inject your way out of bad movement. But you can use biologics to make your movement matter more.”
If you’re considering peptides or exosomes:
- Ask what they’re targeting
- Pair them with a strong rehab plan
- Work with providers who can explain the why and not just the how
FREE DOWNLOAD
Start Optimizing Your Stem Cell Recovery Today with this Recovery Guide!
Recommended Podcast
Similar Articles
- How Stem Cell Therapy Supports Healing and Performance
- Regeneration Meets Rehab in Panama
- The Evolution of PRP
References
Abd El-Aziz, T. A., El-Morsy, A. M., El-Sherbiny, M., & Elgendy, H. (2022). Peptide-based therapeutics: Emerging trends, challenges, and future perspectives. Drug Discovery Today, 27(8), 2134–2148.
Andersen, A. J. C., Holst, J. J., & Christensen, M. B. (2018). Pharmacokinetics of peptide drugs: Challenges and solutions. European Journal of Pharmaceutical Sciences, 115, 93–100.
Baiula, M., Spampinato, S., & Gentili, F. (2020). Emerging peptide therapeutics: Innovation, delivery, and clinical translation. Frontiers in Pharmacology, 11, 611.
Fosgerau, K., & Hoffmann, T. (2015). Peptide therapeutics: Current status and future directions. Drug Discovery Today, 20(1), 122–128.
Goyal, R., & Tripathi, S. K. (2023). Advances in oral peptide drug delivery systems: Overcoming biological barriers. Journal of Controlled Release, 354, 408–423.
Kang, E. A., Han, K. M., & Lee, J. Y. (2021). Intranasal delivery strategies for peptide and protein therapeutics. Pharmaceutics, 13(10), 1591.
Sikiric, P., Rucman, R., Turkovic, B., et al. (2018). Stable gastric pentadecapeptide BPC 157: Novel therapy in gastrointestinal and musculoskeletal healing. Current Pharmaceutical Design, 24(18), 1978–1990.
Sikiric, P., Seiwerth, S., Rucman, R., et al. (2020). The role of the pentadecapeptide BPC 157 in angiogenesis and tissue repair. Biomedicine & Pharmacotherapy, 130, 110506.
Sullivan, R., & Rothman, R. B. (2023). Peptides in sports medicine: Evidence, regulatory concerns, and ethical implications. Sports Medicine, 53(4), 765–779.
U.S. Food and Drug Administration. (2023). Certain bulk drug substances for use in compounding: Risk-based safety review.
Van Dorpe, S., Bronselaer, A., Nielandt, J., et al. (2012). Drug delivery of peptides: Challenges and opportunities. Drug Discovery Today, 17(9–10), 475–482.


