Read: 9 minutes
Write: 0 minutes
Watch:
When I roadmap and reverse engineer a rehab plan, I’m always working from two vantage points at once: Where the athlete needs to end up, and where the biology will realistically let us go next.
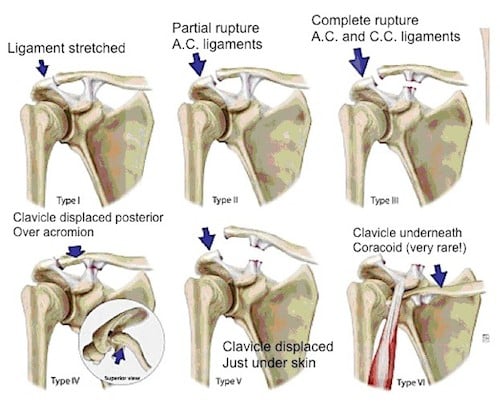
With AC separations—especially Grade III—the process requires clarity, patience, and a deep understanding of the natural history of AC injuries. A cyclist presents a unique case: not an overhead athlete, not a collision athlete, but someone who loads the upper quarter through handlebars, deceleration moments, trunk lean, weight shifting, and high-volume endurance demands.
This lesson walks you through how I reverse engineer the plan and build the roadmap, using this exact case: A cyclist with a Grade III AC separation, MRI imaging, multiple surgical consults, and ultimately—no surgery.
Reverse Engineering: Start With the End Goal
The end goal drives everything. For this athlete, the goal isn’t just “pain-free ADLs.”
The goal is:
- Full return to long-distance cycling
- Pain-free weight bearing through handlebars
- Shoulder girdle capacity to absorb vibration, steering torque, and repetitive small-amplitude perturbations
- Scapular and AC mechanics that do not deteriorate over long-duration rides
- Psychological readiness and confidence (underrated but essential)
And importantly: Return without compensation patterns that create downstream wrist, elbow, neck, or thoracic dysfunction.
Informed by the Evidence
Current research confirms that, for most Grade III AC separations, long-term functional outcomes are equivalent between conservative and surgical care, with surgery providing better cosmetic alignment but higher complication rates.
Return-to-sport rates are excellent across the board—even after surgery—with 89–100% of athletes returning to their sport.
And the newest AC instability frameworks emphasize that Grade III injuries behave along a spectrum—Type IIIA (stable) to Type IIIB (unstable/horizontal instability)—and some IIIA patients truly thrive conservatively.
Our cyclist fits the IIIA profile: Stable radiographs, no horizontal instability on imaging, and no persistent scapular dysfunction.

Step 1: Define the End Goal With Precision
1. Performance Goal
Return to multisurface cycling at pre-injury distance and intensity with stable scapular mechanics and no upper-quarter fatigue.
2. Functional Goal
Handlebar weight-bearing without protective shrugging, excessive elbow flare, or loss of rib-cage control.
3. Structural Goal
A resilient AC joint capable of tolerating long-duration vibration, micro-perturbations, and load transfer between trunk, scapula, and distal upper extremity.
4. Psychological Goal
Confidence in loading the shoulder, especially during standing climbs and emergency maneuvering.
5. Objective Metrics
- Pain ≤ 1/10 during all cycling tasks
- Symmetrical scapular upward rotation and posterior tilt
- 90–100% strength symmetry on dynamometry (horizontal adduction, ER/IR, lower trap, serratus)
- Full tolerance for AC joint compression tests
- Plank variations ≥ 60–90 sec without AC discomfort
- Handlebar pressure mapping (if available) showing symmetrical loading
Step 2: Work Backwards From the Goal
Just like your hamstring example, we break the final goal into milestones that work in reverse:
Return to Sport (Cycling): 12–16 weeks
Full-distance, varied terrain, pain-free, stable scapular mechanics.
Athletes with Grade III injuries managed conservatively demonstrate fast return-to-work and sport timelines in research—often faster than surgical cohorts. What_is_the_prognosis_of_conser…
Return to Performance: 8–12 weeks
Standing climbs, sprints, and high-output intervals without AC discomfort.
Return to Training: 4–8 weeks
Outdoor rides at sub-max intensities; full tolerance for weight-bearing through handlebars.
Restore Local Qualities: 2–4 weeks
AC joint loading tolerance, scapular stabilization, posterior chain and trunk integration.
Restore Homeostasis: 0–2 weeks
Pain control, swelling reduction, restoring sleep, rib cage and scapular positioning.
This backward breakdown forces clarity:
If the final goal is load tolerance on the bike, we must master scapular control, AC joint compression tolerance, and shoulder-to-core force transfer long before we ever return the athlete to the road.
Why Reverse Engineering Works in AC Injuries
Reverse engineering respects:
- Biological timelines of AC ligament healing
- Acute stage: inflammation and pain
- Subacute: collagen deposition and early scar
- Remodeling: dynamic load tolerance over weeks to months
(The AC ligament starts healing quickly but takes months to fully adapt—highlighted in the literature on early healing response.)
- Scapular mechanics as the “symptom amplifier”
Research shows that unresolved scapular dyskinesis persists in up to 70% of chronic Type III injuries—even after “successful” conservative rehab. This is why the movement foundations matter. - The cyclist’s unique demands
Long-duration vibration. Small-amplitude perturbation control. Fixed hand position → fixed load into AC → requires exceptional endurance in the trapezius, serratus, and AC capsule.
Roadmapping: Multiple Routes, One Destination
Reverse engineering sets the path. Roadmapping accounts for reality. Think of it like ride navigation: one route is ideal, but hills, weather, and detours mean we need alternatives.
Primary Route (Ideal)
- Early symptom reduction →
- Scapular control →
- Closed-chain loading →
- Handlebar tolerance →
- Outdoor rides →
- Intensity and duration buildup
This mirrors the predictable timelines seen in conservative care outcomes for Grade III injuries.
Alternate Route A:
If AC joint remains irritable during closed-chain loading: Shift to isometrics, rib-cage control, and deltoid-dominant patterns before reloading the AC joint.
Alternate Route B:
If scapular dyskinesis persists (III B–like behavior): Delay cycling return; emphasize posterior tilt and upward rotation drills, serratus integration, and trunk rotation control.
Alternate Route C:
If cyclist develops secondary symptoms (neck, wrist, opposite shoulder):
Re-balance kinetic chain: thoracic mobility, hand center-of-pressure work, shock absorption strategies.
Real-Time Adjustments
Roadmapping uses clinical checkpoints:
- Pain response
- AC joint compression/shear tolerance
- Scapular control during humeral elevation
- Strength benchmarks
- Functional tasks (planks, carries, cycling posture tolerance)
Just like your hamstring roadmap, these metrics help you decide when to stay the course—or reroute.
Biological Timelines as Your Compass
Inflammatory Phase: Days 0–7
The literature shows that AC and CC ligaments initiate an immediate inflammatory cascade following injury—similar to other dense connective tissues. Histologic studies demonstrate rapid recruitment of fibroblasts and early granulation tissue in the first several days. This early response is part of why both conservative and surgical cases can achieve high healing rates when managed appropriately.
Clinical implications:
- Prioritize pain modulation and gentle scapular assistance.
- Avoid provocative cross-body loading and heavy compressive forces.
- Rebalance rib cage mechanics early—this reduces secondary scapular dyskinesis.
- Begin isometrics in supported positions as tolerated (early neuromuscular preservation).
This period is about controlling chaos and ensuring the athlete doesn’t develop protective motor patterns that will be hard to unwind later.
Proliferative Phase: Weeks 1–3
This is the window where the literature is most compelling. Multiple studies show that if surgery is performed within this timeframe for high-grade injuries, ligament healing is stronger and more predictable. The reason?
The AC and CC ligaments demonstrate an “early and dynamic healing response” with active collagen deposition and early organization of scar tissue.
Even in nonoperative Grade III injuries, this phase is where stability begins to improve—if we load appropriately.
Clinical implications:
- Begin structured loading, but remain sub-threshold.
- Emphasize serratus, lower trap, and rotator cuff isometrics.
- Introduce closed-chain loading at low amplitude (hands supported, no deep compression).
- Avoid excessive shear—this phase is not the time for end-range horizontal adduction or aggressive elevation.
- Restore thoracic rotation early to prevent compensatory scapular internal rotation.
This is the phase where the roadmap starts to diverge depending on whether the athlete demonstrates a IIIA (stable) or IIIB (unstable/horizontal) pattern.
Early Remodeling Phase: Weeks 3–6
By 3–6 weeks, MRI and biopsy studies confirm that the ligaments are laying down progressively more organized collagen fibers. The healing tissue is still immature but now capable of distributing load more efficiently. Studies show excellent outcomes for both conservative care and surgery by this stage when early management is appropriate.
Clinical implications:
- Increase closed-chain work: plank variations, quadruped, wall-supported loading.
- Start low-amplitude perturbation drills to challenge AC stability.
- Introduce handlebar-loading simulations for cyclists with graded pressure exposure.
- Begin humeral elevation strengthening with scapular assistance.
- Continue to address any signs of scapular dyskinesis aggressively—this is the window where it becomes biologically easiest to correct.
The athlete should feel measurably more “trust” in the shoulder by this point.
Late Remodeling Phase: Weeks 6–12
Ligament healing now enters its long arc of progressive collagen cross-linking and alignment. The literature consistently shows that functional outcomes by 3–4 months are excellent across both operative and nonoperative care for Grade III injuries.
Biomechanically, the joint is not “fully healed” yet—but it is load-tolerant.
Clinical implications:
- Progress to higher-intensity closed-chain loading (planks, downward dogs, long-duration supports).
- Integrate multi-planar and higher velocity perturbation strategies.
- For cyclists: simulate climbing, sprinting, descending, and extended handlebar compression.
- Reintroduce sport-specific volume and intensity.
- Begin full return-to-training pathways.
This is the point where an athlete should transition from protecting the joint to challenging it.
Maturation Phase: 12 Weeks – 12+ Months
Across multiple studies, return-to-play after surgical reconstruction typically occurs between 4–6 months, matching the biology of late-stage ligament maturation. Nonoperative Grade III cases follow a similar biological trajectory for tissue adaptation, even though the cosmetic appearance may differ.
By this point, collagen is reorganizing into a more ligament-like structure, load tolerance improves, and functional outcomes continue progressing.
Clinical implications:
- Full training, full intensity.
- High-load scapular stability, dynamic steering control, and endurance.
- Maintenance programming to prevent recurrence or compensatory overload (especially cervical spine, ribs, and trunk).
- Address the long-term risks: persistent deformity doesn’t harm function but can be psychologically relevant; chronic scapular dyskinesis—if not addressed early—may persist.
Combining Reverse Engineering + Roadmapping in This Case
Here’s how the two philosophies work together:
Reverse Engineering gives the structure:
We know the ultimate performance goal and backward-plan all milestones.
Roadmapping provides adaptability:
We build multiple paths depending on:
- Pain response
- AC joint irritability
- Scapular compensation
- MRI or imaging findings
- Psychological tolerance
- Cycling demands (terrain, bike fit, duration)
This hybrid strategy ensures the plan stays both anchored and adaptable.
Key Performance Indicators (KPIs) for This Case
- AC Joint Tolerance
- Compression test
- Cross-body adduction
- Plank loading
- Handlebar simulation tests
(Conservative care shows equivalent long-term outcomes to surgery when these metrics normalize.)
- Scapular Mechanics
Upward rotation
Posterior tilt
Controlled internal rotation under load
(Poor mechanics are linked to chronic dysfunction in Type III injuries.) - Strength
Horizontal adduction
Lower trap/serratus
Rotator cuff endurance
Symmetry ≥ 90–100% - Cycling Posture Endurance
Sustained isometric trunk + shoulder loading
30–60 min cycling tolerance before fatigue or AC irritation - Psychological Readiness
Confidence descending, sprinting, and standing climbing
Conclusion
Reverse engineering gives you the destination and the mile markers.
Roadmapping lets you adapt the path while respecting biology and performance.
For Grade III AC separations—especially in non-overhead athletes like cyclists—conservative care remains a powerful, evidence-supported pathway with excellent long-term outcomes, minimal complication risk, and predictable timelines.
The key is understanding the nuance: scapular behavior, rib cage mechanics, AC joint loading tolerance, and the unique demands of cycling.
Master these principles and you’ll navigate the gray space with confidence—and return your athletes not just to baseline, but beyond it.